
The Whipple procedure is one of the most common surgical treatment for curing pancreatic cancer. But before explaining about that- here is a look at what the pancreas does and all about pancreatitis.
The pancreas, often referred to as the sleeping tiger, is an important organ and it has a lot of functions. It is a digestive organ, helps digestion of fats, proteins, and carbohydrates by secreting many enzymes. It is an endocrine organ. It secretes insulin, which is of fundamental importance in the handling of glucose. If the pancreas is not functioning properly, the patient is at risk of being diagnosed with diabetes.
It is situated in the abdomen behind the stomach. It spreads behind from the duodenum on to the left and it is described as ‘it hugs the duodenum, rolls over the spine and kicks the spleen’.
Ducts in the gland help secretion of enzymes while hormones are directly released into the blood. The main duct opens into the duodenum in the ampulla of Vater and there it joins the bile duct. Hence blockage there can lead to obstruction of both pancreatic and biliary ducts. Sometimes there can be anomalies in the ductal pattern.
What is pancreatitis?
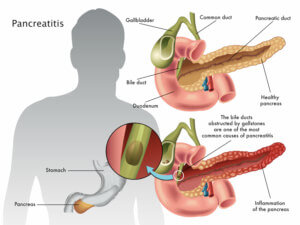
Pancreatitis is an inflammation of the pancreas. The two major causes of pancreatitis are alcohol ingestion and gall stones. Alcoholic pancreatitis is common in men and gall stone-induced pancreatitis is common in women.
Gall stones impacted in ampulla of Vater and reflux of bile in the pancreatic duct causes pancreatitis. Biliary tract disease and alcoholism account for more than 80% of hospital admissions for acute pancreatitis.
Pancreatitis is classified as either acute or chronic. Acute pancreatitis presents with severe abdominal pain. The pain is so severe and unrelenting that it can be mistaken for any of the acute abdominal conditions that require immediate surgery. Chronic pancreatitis is characterized by irreversible and progressive changes in the pancreas that results in a serious loss of exocrine and endocrine pancreatic function and deterioration of the pancreatic structure.
Pancreatitis occurs when pancreatic enzymes start digesting itself and produce a severe reaction. Amylase the enzymes that help digestion of carbohydrates in food become active inside the pancreas and start digesting the pancreas. This enzyme is liberated in the blood and the blood level of amylase is increased a hundred folds.
On entering the systemic circulation, these activated enzymes and toxins increase capillary permeability throughout the body and may produce shock (fall of blood pressure). If ARDS (Adult Respiratory Distress Syndrome) occurs assisted ventilation with positive end-expiratory pressure may be required. When the disease is confined to the pancreas the patient recovers well but when multiple organ failure occurs the outlook is grim.
The pain is usually very severe and in some the disease progresses rapidly on to develop multiple organ failure. Usually the kidneys, lung, clotting system and liver fail. Infection complicating pancreatitis can produce severe, early multiple organ failure.
In gallstone induced pancreatitis gall stones impacted in bile duct needs to be extracted to facilitate the flow of pancreatic secretions. The gall bladder also needs to be removed. The surgical removal of gall bladder can be timed at a later date after the inflammation of the pancreas has subsided. Laparoscopic removal of gall bladder is usually performed.
Pancreatic duct disruption may cause ascites (fluid in the abdomen). When the fluid collection is confined to the space behind the stomach it is called pseudo cyst. These cysts may require surgical correction.
Serum amylase and lipase concentrations increase on the first day of acute pancreatitis and return to normal in 3 to 7 days. The patient may develop mild jaundice because of compression of the common bile duct.
Ultrasound of the pancreas and CT scan help in diagnosis. If CT shows only mild pancreatic edema, the prognosis is excellent; a markedly swollen pancreas denotes a more severe prognosis.
Chronic pancreatitis:
Chronic pancreatitis most commonly results from alcoholism and gall stones. In India, idiopathic calcific pancreatitis occurs among children and young adults. Tapioca in food is blamed for this condition. Progressive destruction and fibrosis produce symptoms.
Persistent abdominal and back pain with diabetes, malabsorption makes one suspect chronic pancreatitis. Back pain may be mistaken for spinal pain and alcoholics complaining of persistent pain may be dubbed as neurotics. The majority being alcoholics, poor compliance of treatment is the rule.
Structural abnormalities can be visualized by plain x-ray of the abdomen, abdominal ultrasound or CT and ERCP. The pancreatic duct is irregularly dilated and inadequate drainage of pancreatic secretion leads to pain. There are various test to ascertain the digestive function of the diseased pancreas.
A relapse of chronic pancreatitis may require treatment similar to that of acute pancreatitis. The patient must stop alcohol intake. Pancreatic digestive enzymes may be supplemented. Insulin is required to treat diabetes mellitus caused by chronic pancreatitis.
The pancreatic pseudocyst, if persisting needs surgery. The dilated ductal system of the pancreas is drained by surgery and this gives good pain relief.
Patients with chronic pancreatitis are at increased risk of pancreatic cancer. In chronic pancreatitis, the pancreatic gland develops mass and it is difficult to differentiate it from cancer of the pancreas. It may require biopsy and if still inconclusive surgical removal is done. Pancreatitis especially the chronic variety needs correct assessment, continual therapy and above all a compliant patient.
Pancreatic cancer- Causes and Risk Factors
Pancreatic cancer is a disease in which malignant (cancer) cells form in the tissues of the pancreas. Death of Apple co-founder Steve Jobs due to pancreatic cancer has brought into focus this rare and aggressive form of cancer, which is causing concern in India following a rise in incidence of the disease.
Where is the Pancreas situated?
The pancreas is a gland about 6 inches long that is shaped like a thin pear lying on its side. The wider end of the pancreas is called the head, the middle section is called the body, and the narrow end is called the tail. The pancreas lies behind the stomach and in front of the spine.
What is the function of the Pancreas?
The pancreas has two main jobs in the body:
To produce juices that help digest (break down) food.
To produce hormones, such as insulin and glucagon, that control blood sugar levels. Both of these hormones help the body use and store the energy it gets from food.
The digestive juices are produced by exocrine pancreas cells and the hormones are produced by endocrine pancreas cells. About 95% of pancreatic cancers begin in exocrine cells.
How common is Pancreatic cancer?
According to medical experts, pancreatic cancer is ranked fourth in cancer-related deaths in the US, after lung, prostate and colorectal cancer. Traditionally it is a male- predominant cancer, however the recent increase in the incidence of Pancreatic Cancer in women over the last three decades is because of increased smoking behaviour in women.
The incidence of Pancreatic cancer is highest in African -Americans. It has a negligible 5 year survival rate of 6.7%. At the time of diagnosis, 52% of patients have distant disease, 26% have regional spread. The global prevalence rate of pancreatic cancer is 9 cases per 100,000 people. The cancer form has seen a rise in India in recent times.
According to Delhi Cancer registry, Mizoram in India has the highest prevalence of pancreatic cancer. The incidence of Pancreatic cancer in India is 0.5-2.4 per 100000 in men.
Risk Factors for Pancreatic Cancer:
Anything that increases your risk of getting a disease is called a risk factor. Having a risk factor does not mean that you will get cancer; not having risk factors doesn’t mean that you will not get cancer. Risk factors for pancreatic cancer include the following:
- Age > 50 years
- Smoking- 74% increased risk of Pancreatic cancer
- Obesity- 12% of all pancreatic cancers are attributed to overweight and obesity, Risk increases by 10% for a 5 point increases in BMI (Body Mass Index) score
- Diet- Increased consumption of processed meat and saturated fats.
- Long-standing diabetes- especially, newly diagnosed diabetics > 50 years of age.
- Chronic pancreatitis- 1% of pancreatic cancer cases linked to chronic Pancreatitis.
- Hereditary Pancreatic Cancer- 5-10% of cases of Pancreatic cancer.
Hereditary pancreatitis runs in families and usually occurs at a young age, often before the age of 30. These patients have a risk that is 50-60 times greater than expected. Certain hereditary conditions, such as hereditary pancreatitis, multiple endocrine neoplasia type 1 syndrome, hereditary nonpolyposis colon cancer (HNPCC; Lynch syndrome), von Hippel-Lindau syndrome, ataxia-telangiectasia, and the familial atypical multiple mole melanoma syndrome (FAMMM) are risk factors for Pancreatic cancer.
Symptoms of pancreatic cancer:
- Jaundice (yellowing of the skin and white of the eyes).
- Pain in the upper or middle abdomen and back.
- Weight loss for no known reason.
- Loss of appetite.
- Fatigue.
Why is it difficult to detect Pancreatic cancer in the early stages?
There aren’t any noticeable signs or symptoms in the early stages of pancreatic cancer. The signs of pancreatic cancer, when present, are like the signs of many other common gastrointestinal illnesses.
The pancreas is hidden behind other organs such as the stomach, small intestine, liver, gallbladder, spleen, and bile ducts, hence routine USG (ultrasound) abdomen does not pick up early lesions in the Pancreas, detailed investigations like CT abdomen or Endoscopic Retrograde Cholangio Pancreatography (ERCP) are required.
Whipple’s Surgery- Pancreo Duodenectomy

Early malignancies of the pancreas are usually treated by Whipple’s operation, medically called PANCREO DUODENECTOMY. This involves resection of the head of the pancreas and its adjoining duodenum and common bile duct. Various advances in gastrointestinal surgery have contributed in achieving lower mortality and morbidity by many surgeons.
This highly demanding procedure requires the highest level of surgical training and excellent technical skills.
The history of this pancreatic – duodenectomy extends from the late 19th century. In 1898, Halsted was the first to successfully remove the head of the pancreas.
In 1935 Dr Allen Whipple, Parsons and Mullins performed the first reported total duodenectomy as a part of his two-stage procedure. It was modified by Waugh & Clagett in the present form.
The excellent outcomes in the recent past have been very successful has led to an increasing number of centres and surgeons in performing pancreaticoduodenectomies on a daily basis. A major factor in the success of the Whipples procedure was their effort to prevent pancreatic leak.
Recent advances in surgery advances and critical care have resulted in the reduction of early mortality to less than two percent.